INTRODUCTION
Men’s ice hockey is growing in popularity with more than 1.6 million athletes in 79 countries playing the sport annually.1 Although players wear well-developed protective gear, ice hockey is among the team sports with the highest injury incidence rate, particularly those of traumatic origin.2 Several reasons may explain the sport’s high traumatic injury rate. In men’s ice hockey, body checking is permitted and collisions between players may also happen incidentally. Moreover, fighting is an accepted component of the game in many professional leagues. Other sources of trauma include the aggressive use of carbon-made sticks, collisions with rigid boards or goals, lacerations incurred by skate blades, and contusion due to blocking of the vulcanized rubber-puck with the body. Traumatic injuries are of particular concern at elite levels, where players can skate at speeds close to 50 km/h and can shoot the puck at velocities above 150 km/h.3 Consequently, the internal and external forces generated by the athlete can be significant and lead to severe injuries.4 Professional athletes may also be particularly prone to overuse injuries as they are required to play three times a week over a seven to nine month competitive season.5 In summary, the highly traumatic nature of the sport, the congested match schedule and the competitive environment of the professional sport are all factors that seem to influence both the traumatic and overuse injury rate of ice hockey players at elite levels.6 In this context, a thorough overview of the injury incidence profile at professional levels may help the support staff to prioritize the application of risk reduction measures within teams to promote safer sport participation. Although a discrete number of studies have described the incidence and types of ice hockey related injuries in different professional leagues and competitions, most of the literature on the subject consist of case report or case series.7–10 Moreover, published research has often focused on a particular injury type or on a single anatomical location, such as concussions or hip/groin problems.10,11
Therefore, the primary objective of the was to conduct a systematic review to quantify the injury incidence rates in professional male ice hockey. The secondary objective was to carry out a sub-analysis to determine the profile of injuries, with specific focus on anatomical location, mechanism, type and severity.
METHODS
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) protocol was followed to conduct this study.12,13 The PRISMA checklist is presented in Appendix I.
Information Sources and Search Strategy
Eligible studies were identified by using a systematic computerized search performed between February 1st and November 30th 2022. PubMed, CINAHL, Web of Science and ProQuest-Sport medicine & Education Index databases were consulted. Pro-Quest Dissertation and Thesis was used to search potential unpublished studies . A two-compartment additive search with the following terms was created: (“Ice hockey” OR “Winter sport*” OR “Winter Olympi*”) AND (“Injur*” OR “traum*” OR “strain*” “sprain*” OR “wound” OR “fracture*”). Additionally, the subject headings terms “hockey”, “athletic injuries”, “wounds and injuries” and “epidemiology” were included. A complete scheme of the search strategies for each database is provided in Appendix II. The reference lists of the review articles recovered were manually searched to screen for potentially eligible studies not captured by the computerized searches.
Two reviewers (MC and CR) independently read the titles and the abstracts of the articles identified by the search strategy and those that did not meet the inclusion criteria were excluded. Thereafter, full text articles were reviewed for final exclusion. A third external reviewer (KT) was consulted to resolve discrepancies throughout the selection process as needed.
Eligibility Criteria and Study Selection
To be included in this systematic review, the studies had to fulfill the following criteria:
-
Participants had to be professional male ice hockey players; that is athletes had to play for a team that was engaged in professional national leagues, professional tournaments or winter Olympics
-
Injuries had to occur because of ice hockey training, professional ice hockey championships, professional international tournaments or winter Olympics.
-
Eligible studies had to report the number of missed training or competition days as result of injury.
-
Injury incidence rate must have been reported, or enough data provided to calculate it using standardized equations.
-
Overall injury incidence rate as a result of ice hockey participation had to be reported.
-
Studies had to be prospective or retrospective cohort studies available in full text and published in English before the 1st of November 2022.
Studies with data pertaining to non-elite competitions or regarding only female ice hockey players were excluded. Research with data including both elite and amateur competitions or male and female ice hockey were excluded unless data for the elite male cohort could be extracted. Studies adopting injury definitions other than time loss were excluded. Research that focused only on a particular injury type or on a single anatomical location were not included.
Data Extraction
Data from selected studies were extracted using a tailored standardized Microsoft Excel (version 16.29, 2019) spreadsheet. Data were grouped into three categories:
-
General study information: authors, year of publication, length of observation, location.
-
Study population: sample size
-
Epidemiological information: injury incidence rate (overall vs training vs match injuries rates), anatomical location (lower extremities vs upper extremities vs trunk vs head and neck), mechanism of injury (traumatic vs non-traumatic), type of injury (bone vs joint vs muscle-tendon vs laceration vs contusion vs concussion vs others), severity of injury (1-7 days vs 8-28 days vs >28 days).
Quality Evaluation
Two scales were used to assess the quality of the selected studies. External validity was assessed according to a modified version of the Newcastle Ottawa scale (NOS) for cohort studies.14 In particular, items number two (selection of the non-exposed cohort) and number five (comparability of cohorts on the basis of the design or analysis) were excluded as all participants of the selected studies were exposed to ice hockey participation. Reporting quality was assessed according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement, which contains the essential items that should be described in observational epidemiological studies and its extension.15 In particular, the STROBE Sports Injury and Illness Surveillance (STROBE-SIIS), which contains recommendations from the International Olympic Committee regarding observational studies in sports medicine was used.16 STROBE-SIIS adds 16 sub-items to the 34 included in the original STROBE checklist, therefore a maximum score of 50 indicates that the article fulfilled requirements for high-quality publication.
Synthesis of Results
Data were aggregated and a narrative critical analysis was conducted. The incidence of injuries during games and training were analyzed separately. A sub-analysis of the same studies was conducted in order to determine the most frequent anatomical location, mechanism, type and severity of injury. A meta-analysis was not attempted because epidemiologic information was not reported consistently among the selected studies.
RESULTS
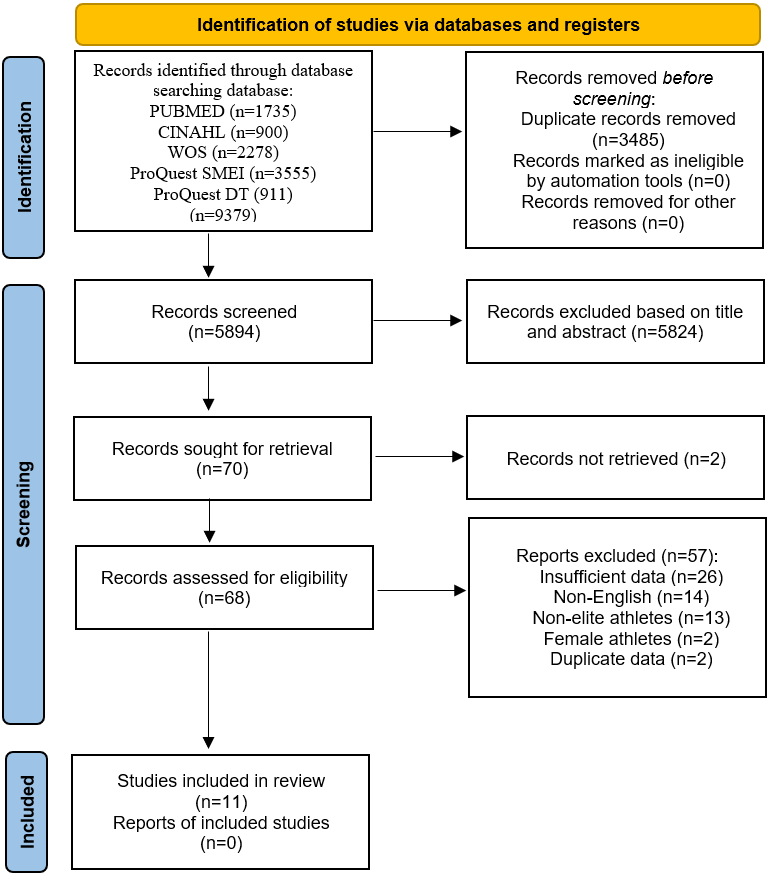
A total of 9379 references were identified after the search process, of which 3485 were excluded as duplicates. Five-thousand, eight hundred and twenty-four studies were eliminated after reading the title and the abstract as the inclusion criteria were not met. Additionally, two articles were not retrieved. Therefore, the full text of 68 articles was reviewed. Twenty-six items were excluded due to a lack of reported data exposure and consequently the incidence rate could not be calculated. Twenty-nine studies were excluded for not meeting criteria and two other articles used duplicate data. Eleven articles were included in this systematic review. The flow chart of the selection process is presented in Figure 1.

Quality Assessment
All studies selected for this systematic review had a low bias risk with 10 possessing the maximum score on the points modified NOS (0 to 6 points). All studies collected data prospectively through a health staff member except Jorgensen et al.,17 where athletes had to retrospectively self-complete a questionnaire on injuries sustained during the past season. For this reason, Jorgensen at al.17 had a modified NOS score of 5. Appendix III displays the results obtained from the modified NOS for all selected articles. With regard to the reporting quality of the studies, the results obtained with the STROBE-SIIS quality scale are presented in Appendix IV. The mean score was 33 (minimum: 28, maximum: 38), which represents a compliance of 66% of the items. None of the studies reported ethical committee approval and source of funding and study registration was reported only by Brunner et al.18 Moreover, none of the studies acknowledged potential biases and the validity of the collection tools was only reported by one study.18 Re-injury and injury burden were not calculated in any of the selected studies.
Descriptive Characteristics of the Selected Studies
All studies were published between 1986 and 2020 and the length of observation ranged from 1-10 years. One study analyzed the epidemiology of injury during international competitions (winter Olympics)19 and two studies reported the injury trends in a national team.20,21 The remaining studies focused on professional national leagues. The total sample size was 8712 athletes and the total number of injuries was 7502. Table 1 shows the main characteristics of each of the selected studies.
Injury Incidence rate
The injury incidence rate during matches was reported by 10 studies and ranged from 38 to 88.6 injuries/1000 hours of exposure.17–24,26,27 Five studies included the injury incidence rate during training, with values between 0.4 and 2.6 injuries/1000 hours of exposure.17,18,22,24,26 Only three studies reported the overall injury incidence rate, which ranged from 2.14 to 5.6 injuries/1000 hours of exposure.17,24,25 Table 2 shows the injury incidence rate data for each of the selected studies.
Anatomical Location
As shown in Table 3, nine studies reported the anatomical location of the injuries.17–19,21–23,25–27 Five studies found that the lower extremities were the most affected by injuries, representing 27%-53.7% of all injuries,18,22,23,25,26 whereas four studies reported that injuries to the neck and head were the most common, representing 28%-50% of all injuries.17,21,27,28 Injuries to the upper extremities ranged from 12% to 25.5% and those to the trunk ranged from 7.8% to 26% of all injuries. The largest difference between study results was found in the neck and head category which accounted for 6.3% of total injuries in the study of Lorentzon et al.22 but represented 50% in another study by Lorentzon et al.21 Only two studies analyzed traumatic and overuse injuries separately.18,22 Both showed that the knee was the anatomical area most affected by trauma while the hip/groin region was the most prone to overuse issues.18,22
Mechanism of Injury
The mechanism of injury was reported by eight studies (Table 4).18–23,26,27 In all of these studies, the primary cause of injury was trauma, with values between 76% and 96.6%. Non-traumatic injuries ranged from 0% to 24%. Body checking and collision were the main cause of injury in six studies.18–23 Two studies found stick contact as the most prevalent cause.25,27 Three studies analyzed foul play and reported that it was the cause of 8-50% of injuries .21,22,27
Injury Type
As shown in Table 4, nine studies reported the type of injury that occurred during the observation period.17–19,21,22,24–27 Four studies found contusions as the most prevalent injury type, whereas three studies reported lacerations,17,21,22,24 one study joint-related injuries25 and one study muscle-related injuries to be the most common.18 In particular, contusion accounted for 15%-46% of all injuries and laceration for 1%-26.8%. Fractures represented 4.7%-14.4% of all injuries, joint sprains or dislocation accounted for 12%-33% and muscle strain for 9%-24%. Concussions accounted for 18% of all injuries in the study of Brunner et al.,18 while Lorentzon et al. did not observe any cases of concussion.21
Severity of Injury
Seven studies reported the severity of injuries (Table 5).17,19,22,24–27 Five studies found that the majority of injuries were mild (1-7 days of absence from practices or competitions),19,22,24,26,27 whereas two studies found that the majority of injuries were of moderate severity (8-28 days of absence).17,25 Severe injuries (> 28 days of absence) ranged from 7.8% in the study of Molsa et al.24 to 20% in the study of Ornon et al.25
DISCUSSION
The aim of this systematic review was to quantify the incidence of injuries in professional male ice hockey, while the secondary objective was to carry out sub-analyses to determine the profile of injuries, with particular regard to anatomy, mechanism, severity, location and type of injury. The review shows that professional male ice hockey players are exposed to a substantial risk of injury during match play, while training injuries are less frequent. The majority of injuries are traumatic and severe injuries account for a notable portion of overall injury cases.
Quality of the evidence
All selected studies showed low bias risk for external validity. There was only 66% compliance with the items of the STROBE-SIIS quality scale. It should be noted that the STROBE-SIIS quality scale has only been proposed since February 2020, whereas all the studies included in the present review have been carried out before that date.16
Injury Incidence
The main findings of this study show a match injury incidence of 38 to 88.6 injuries/1000 hours of exposure and a training injury incidence of 0.4-2.6 injuries/1000 hours of exposure. Therefore, professional players have a much higher risk of suffering an injury during a match than during a training session. Compared to other team sports, participation in ice hockey training session can be considered safer, however the aggressive nature of the sport seems to emerge during matches, where a high injury incidence has been reported.29,30 The findings of this study also indicate that professional ice hockey players sustained more injuries when compared to non-professional players where the match injury incidence has been reported to be 13.8 injuries/1000 hours of exposure in the American Collegiate League3 and 4.7 injuries/1000 hours of exposure in the Swiss interregional league.31 Injuries in professional male tournaments also seem more frequent than in women tournaments, where the match injury incidence has been found to be 22/1000 hours of exposure.28 In female hockey, however, full facial protection is mandatory and body checking is not allowed and consequently the risk of injuries is decreased.32,33
Injury Profile
Lower extremity is the anatomical region more frequently injured. In particular, the knee was the joint most affected by traumatic injuries, while the hip/groin complex was the most affected by overuse problems. In this context, it should be noted that knee injury prevention programs have been shown to be effective in several sports.34–37 Unfortunately, however, it is still unclear whether they can prevent traumatic injuries or only non-contact ones.38 Therefore, it would be interesting to implement these programs in ice hockey, where unlike other sports, most knee injuries are traumatic in origin. Regarding hip/pelvic overuse issues, it is important to note that this phenomenon is probably more widespread than what was found in this review where only missed training and competitions were considered. In fact, a recent study found that 48 percent of ice hockey players suffered from non-time loss hip/groin problems during a season, with significantly worse hip and groin function than healthy teammates.39 These findings highlight the need for a proper management of training loads during the off-season, preseason, and in-season.40 Moreover, exercises targeting muscle strength and coordination in the hip, groin, and pelvis have shown promise in reducing pain and improving function.41,42
Body checking and collision with another player represented the major cause of injury. Therefore, disallowing body checking could be considered a reasonable initiative to reduce the number of injuries. This policy has already been introduced in several leagues in youth hockey and in women’s hockey and has proven effective in decreasing injury rates.33,43,44 Other sources of trauma include contact with the stick, the puck, or the skate blades, all objects that have the potential to create contusions and lacerations to the athletes. In order to reduce these injuries, improving protective gear with enhanced with materials that can better absorb external forces and are constructed of cut-resistant fabric should be considered.
Contusions and lacerations represented the most common injury types. Lacerations to the face were particularly common.24,27 These could be prevented by mandating the use of full facial protection. In fact, this measure, already in place for under-18s and in female hockey, has been shown effective in reducing facial injuries.32,33,45
Contusions and lacerations normally heal in a short time, and this can explain why most of the injuries were reported to be of minimal severity. However, fractures, joint and muscle-tendon injuries were also common and may represent a large percentage of those injuries with moderate or severe recovery time. Severe injuries were present in similar proportion to other collision sports.30,46
Limitations
The main limitation of this study is that none of the included articles reported re-injuries. It was therefore not possible to calculate the incidence of these injuries separately. A second limitation is that some of the athletes in the sample of Tegner and Lorentzon27 and in the sample of Petterosn and Lorentzon26 also has a secondary occupation. However, all the players competed in the highest Swedish hockey division and the reported injuries only concerned hockey practices or matches. A third limitation concerns the reporting of concussion injuries, which in some studies account for a substantial portion of the injuries while in others did not.18,21 An agreed definition of concussion was only reached in 2001, so studies published before this date may have recorded concussion in a different category.47
CONCLUSION
In professional male ice hockey, the risk of injury during training is low compared to other sports. However, during competitions, professional male ice hockey players are exposed to a substantial risk of injury, especially to the lower limbs. The vast majority of injuries had a traumatic mechanism, with contusions and lacerations being the most common injury types.
Conflicts of interest
The authors report no conflicts of interest.